





When the state imposes age restrictions on consumption of certain goods and services, potential customers often look for ways to avoid these restrictions. “Border-hopping” refers to the practice of crossing a state’s border from the state that has stricter restrictions to the state with more lenient age policies and is well documented in reference to alcohol consumption and the use of reproductive services (including abortion services). The recent study “Behind-the-counter, but Over-the-border?” by UHERO’s Dr. Inna Cintina applies the same concept to emergency contraception (EC).
EC may effectively prevent unwanted pregnancy if taken promptly after unprotected sexual intercourse. Although some forms of EC were available on an off-label basis for nearly 30 years, it formally received FDA approval on a prescription basis only in the late 1990s. In 2006, the FDA lifted the prescription requirement for women age 18 and older. In 2009, the FDA dropped the age requirement to 17, and in 2013 to 15 years of age.
Since EC efficacy is inversely related to the duration between intercourse and the time it is taken, prescription requirements can make it less effective. Between 1998 and 2006, eight states took steps to relax the prescription requirements, making EC available behind-the-counter* without an age restriction. Washington State was the first state to implement collaborative drug therapy agreements between physicians and pharmacists, essentially increasing the availability of EC. The study “Behind-the-counter, but Over-the-border?” focuses on the Washington state experience and identification of potential spillover effects on neighboring states. The study finds some evidence in support of spillover effects in Idaho, but not Oregon. After accounting for changes in the availability of abortion services, the decrease in fertility rates in Idaho counties with a no-prescription EC pharmacy in close proximity is rather small and models lack sufficient power to detect it.
In Hawaii EC became available without a doctor’s prescription in 2003. Since Hawaii is fairly isolated state, the costs of border-hopping outweigh the potential benefits and spillover effects are unlikely. Figure below shows abortion rate** per 1,000 women age 15-44 in Hawaii, by county of residence.
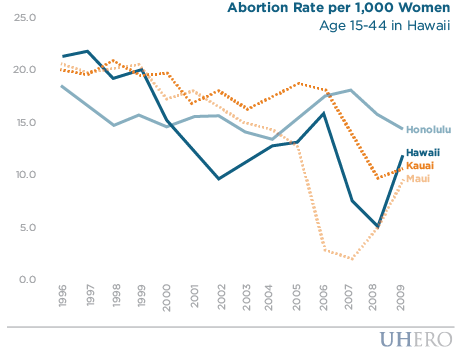
Between 1996 and 2003 abortion rates were declining in Hawaii, Kauai, and Maui counties and were relatively stable in Honolulu County. After 2003, the abortion rate in Maui County continued a decreasing trend. In contrast, for at least two years, abortions rates had increased in Hawaii and Kauai counties. In Honolulu County abortion rates increased sharply after 2004. The dynamic of the county specific rates may have been affected by the availability of reproductive services, pharmacist participation in collaborative agreements, the general dissemination of information among potential customers as well as a number of other factors. A more rigorous analysis is needed to identify the impact of increased availability of EC on fertility rates in Hawaii after 2003.
*A formation of collaborative drug therapy agreements between physicians and pharmacists allowed the pharmacists to make an independent assessment of a woman’s need for EC and a decision to dispense EC without a doctor’s prescription. But he still had to follow the established drug therapy protocol therefore the EC was not on the shelves.
**Abortion rate is defined as the total number of abortions in a county divided by the female population age 15-44 in that county.
– Inna Cintina